Introduction
The chosen subject matter for this vital evaluation is “Addressing Maternal Mortality in India.” This file targets to comprehensively investigate the general public health landscape surrounding maternal mortality in India, dropping mild at the contributing factors, winning interventions, and the alignment of policies with the evidence on causes. Maternal mortality is a pressing difficulty that demands immediately attention and strategic interventions to beautify the overall well-being of women in India.
The focal point of this document is to significantly examine the multifaceted aspects of maternal mortality, encompassing the socio-financial determinants, healthcare infrastructure, and policy frameworks. by way of drawing on theories and fashions included in the public health module, the document seeks to offer a nuanced perception of the basis causes and propose evidence-based interventions that may serve as a foundation for destiny public fitness practices in India.
Through a vital analytical approach, the document will explore the existing statistics on maternal mortality, investigate the efficacy of current interventions, and evaluate the ethical dimensions surrounding maternal fitness guidelines. This research is critical to inform public fitness practitioners, policymakers, and applicable stakeholders about the gaps and opportunities for improvement in addressing maternal mortality inside the Indian context.
Background
Maternal mortality in India stands as a critical public fitness problem, reflecting the complex interaction of socio-financial, cultural, and healthcare factors. The astonishing quantity of maternal deaths increases alarms about the overall nicely-being of female in the country, necessitating a complete exploration of the underlying causes and capacity interventions (Meh et al., 2022).
From a public fitness perspective, maternal mortality is a multifaceted issue that is going beyond medical care, encapsulating broader social determinants. the general public health module classes 1-2 supplied foundational information on how fitness is stimulated by different factors, emphasizing the significance of appreciation the “causes of the causes,” a notion highlighted by Sir Michael Marmot (Hamal et al., 2020). within the case of maternal mortality in India, these causal factors make bigger past clinical complications to encompass inadequate get admission to to fine healthcare, socio-financial disparities, and cultural norms affecting ladies’s autonomy and selection-making (Jose, 2018).
records on maternal mortality quotes in India underscore the severity of the difficulty. no matter development in latest years, the us of a nonetheless faces demanding situations in achieving sustainable development goals associated with maternal health. using facts from these classes, it is able to critically examine the data to pick out styles and disparities. as an example, certain regions or demographic agencies can also experience disproportionately better maternal mortality prices, highlighting the need for targeted interventions (Das, 2018).
Furthermore, framing the background includes thinking about global health tendencies. the issue of maternal mortality in India resonates with worldwide demanding situations, aligning with broader discussions on attaining common fitness insurance and decreasing fitness inequities. international tendencies in maternal fitness underscore the interconnectedness of health effects, emphasizing the need for collaborative efforts to deal with not unusual demanding situations throughout countries (Patrick et al., 2022).
The background of maternal mortality in India as a public health situation is formed with the aid of a myriad of items, as elucidated in the early periods of the module. Leveraging this expertise, we are able to critically analyse applicable data, thinking about each nearby and international views to offer a complete basis for addressing maternal mortality inside the Indian context (Khandale and Kedar, 2017).
3. Prevention
Main Causal/Contributory Factors
Maternal mortality in India is deeply rooted in a complicated net of contributing elements that expand some distance beyond the instant healthcare environment. perception and addressing these factors are crucial for the development of powerful prevention techniques.
At the forefront of causal elements is the structural inadequacy of India’s healthcare system. restrained get entry to best maternal healthcare services, particularly in rural regions, exacerbates the hazard for pregnant women. the general public fitness module’s periods 1-2 emphasised the importance of structural determinants in health consequences, aligning with Marmot’s attitude on addressing the “reasons of the reasons.” in the context of maternal mortality, those structural issues include insufficient healthcare facilities, a shortage of skilled healthcare experts, and demanding situations in transportation infrastructure, hindering timely get admission to medical help all through being pregnant and childbirth (Kumari et al., 2019).
Furthermore, socio-monetary disparities and gender-primarily based inequalities play a pivotal role in maternal mortality. women in lower socio-economic strata regularly face barriers in accessing antenatal care, professional birth attendants, and emergency obstetric care. Cultural norms and conventional practices, coupled with constrained decision-making autonomy for girls, further contribute to delays in seeking and receiving suitable healthcare (Singla et al., 2017). This intersectionality of social determinants, as discussed in module periods, underscores the want for interventions addressing the root reasons of maternal mortality.
Inequalities in maternal mortality are stark across regions and demographic organizations. Rural areas witness higher maternal mortality fees due to confined healthcare infrastructure and educational opportunities. additionally, marginalized communities, including scheduled castes and tribes, face disproportionate challenges, amplifying the disparities. spotting these inequalities is essential for tailoring prevention strategies which can be contextually touchy and deal with the unique challenges confronted via exclusive populations (Singh, 2021).
Appreciation the causal elements also calls for an acknowledgment of the broader societal context, wherein women’s health is interconnected with educational possibilities, monetary empowerment, and cultural norms. Integrating this attitude from module periods 1-two, interventions can cross beyond immediately healthcare provision to cope with the social determinants that structure maternal fitness results (Small et al., 2017).
The primary causal elements contributing to maternal mortality in India are deeply embedded in structural inadequacies, socio-financial disparities, and gender-primarily based inequalities. Leveraging insights from the early periods of the module approves for a complete grasp of those elements, forming the idea for powerful prevention techniques that cope with the basis reasons of maternal mortality (Kumari et al., 2019).
Pathogenics and Salutogenics
Maternal mortality in India is intricately linked to the guidelines and political support surrounding reproductive health. An essential assessment of cutting-edge and historic policies offers valuable insights into the efforts undertaken to deal with this urgent public health subject.
Current or Historical Policy/Political Support
India has witnessed a dynamic landscape of rules focused on maternal fitness, reflecting a mix of country wide and state-degree tasks. The country wide fitness challenge (NHM), launched in 2005, contains the Reproductive, Maternal, newborn, baby and Adolescent fitness (RMNCH+A) method, demonstrating a political dedication to improving maternal fitness results (Alam et al., 2020). but, despite those tasks, the ground reality well-known shows gaps in coverage implementation, especially in rural and marginalized groups in which maternal mortality fees continue to be alarmingly high.
moreover, political help for maternal health has visible fluctuations over time. while certain intervals have witnessed heightened attention, others have experienced policy inertia. The socio-political context often influences the prioritization of fitness problems, impacting the sustained commitment to maternal fitness initiatives (Parsekar et al., 2020).
Alignment of Government or WHO Policy with Evidence on Causes
The alignment of rules with evidence at the causes of maternal mortality is a critical determinant in their effectiveness. the public health module, especially the classes on public health coverage and Key Public health organizations, emphasised the importance of proof-based policymaking (O’Neil et al., 2019).
India’s policy landscape, while acknowledging structural and social determinants, often faces demanding situations in translating proof into actionable strategies. the point of interest has traditionally been on medical interventions rather than addressing the root reasons highlighted in Marmot’s framework. The evidence on socio-economic disparities, gender inequalities, and structural inadequacies frequently requires extra comprehensive and included procedures than what is meditated in present regulations (Rajwar et al., 2023).
the arena health enterprise (WHO) provides worldwide hints on maternal fitness, emphasizing the want for a continuum of care, from preconception to postpartum. Assessing the alignment of India’s rules with these international guidelines well-known shows areas where changes are critical, in particular in tailoring interventions to the diverse socio-cultural contexts within the United States (world fitness enterprise, 2018).
Focus of Policy on Societal Change and the Health-Enhancing Environment
Public health policy underscored the significance of regulations that promote societal trade and contribute to a fitness-improving environment. Inside the case of maternal mortality, suggestions want to make larger preceding scientific interventions to tackle societal norms and structural determinants. at the equal time as some insurance policies comment on broader societal modifications, there is room for improvement. initiatives promoting female’s empowerment, schooling, and monetary independence are imperative components of a holistic strategy then once more do not appear to be constantly blanketed into contemporary recommendations (O’Neil, 2019). A shift nearer to insurance policies that cope with the social determinants of maternal mortality is quintessential for sustainable upgrades.
Changes in Policy Direction Over Time
Analysing changes in insurance route by means of the years exhibits the evolving response to maternal mortality. Early insurance policies regularly centered on scientific interventions and get admission to healthcare centers. over the years, there has been an acknowledgment of the desire for an extra complete approach, aligning with worldwide tendencies advocating for built-in maternal health services. however, annoying conditions persist in the steady implementation of rules that replicate these evolving perspectives. Political changes, useful resource constraints, and competing fitness priorities make contributions to the dynamic nature of insurance guidelines (Parsekar et al., 2020). The venture lies in making sure continuity and coherence in insurance frameworks in spite of these stressful situations.
The comparison of pathogenics and salutogenics in the context of maternal mortality in India highlights a blended panorama of insurance plan insurance policies and political support. at the same time as there can additionally be proof of dedication and efforts, gaps persist in translating proof into fine strategies that tackle the basis reasons of maternal mortality. A larger comprehensive, proof-based totally, and covered approach is indispensable to make positive that policies now now not completely align with world pointers then once more moreover make a contribution to societal alternate and a fitness-enhancing environment, in the lengthy run most important to a giant discount in maternal mortality expenses (Alam, 2020).
Public Health Interventions
Maternal mortality in India wants a multifaceted method that encompasses pretty a wide variety intervention, ranging from insurance plan and societal changes to customer-targeted and network-pushed actions. analysing these interventions through the lens of public health fashions, ethical concerns, and a range of quintessential views offers a whole hold close of their strengths and boundaries (Singh, 2021).
Range of Interventions
Policy/Societal Change Interventions:
Guidelines aimed toward societal alternate play a pivotal role in addressing maternal mortality. initiatives promoting women education, empowerment, and financial independence are indispensable components. The Janani Suraksha Yojana (JSY), a conditional cash switch scheme, exemplifies a coverage intervention targeted on growing institutional deliveries. but, the effectiveness of such policies is contingent on addressing underlying social determinants, which include gender inequalities and cultural norms (Mukaruzima et al., 2023).
Client-Centered Interventions
Purchaser-centered Interventions are pivotal in addressing maternal fitness, and the Pradhan Mantri Surakshit Matritva Abhiyan (PMSMA) in India exemplifies such an attempt. This initiative gives loose antenatal care, emphasizing custom-made activity for pregnant ladies. however, its commendable goals, traumatic situations persist, frequently in rural regions. variations in company great and limited accessibility in faraway areas pose precise sized hurdles. Inconsistencies within the implementation of PMSMA can convey about disparities internal the stage of care provided, impacting the usual effectiveness of the intervention. Addressing these annoying situations is vital to make certain that consumer-targeted care turns into a truth for all pregnant female, regardless of their geographic area or socio-economic repute (Jose, 2018).
Community Action Interventions
Community-driven interventions, exemplified through the authorised social health Activist (ASHA) program, play a pivotal role in improving maternal health in India. ASHAs function vital intermediaries, fostering focus and facilitating get admission to healthcare offerings within nearby communities. Their engagement is crucial to promoting maternal nicely-being by means of addressing cultural nuances and limitations which can hinder healthcare usage. however, the effectiveness of these packages’ hinges on elements along with ample schooling, availability of assets, and cultural sensitivity. ensuring that ASHAs are properly-prepared with the necessary abilities, supported by way of resources, and culturally aware is critical for the sustained fulfilment of community-driven interventions (Patrick et al., 2022). through addressing these factors, projects like the ASHA software have the capability to significantly enhance maternal fitness consequences via network engagement and empowerment.
Relating Interventions to Public Health Models
Utilizing public health models aids in understanding and categorizing interventions:
Social Ecological Model
Interventions guided by way of the Social Ecological model intention to address maternal fitness challenges across various ranges, acknowledging the interconnected nature of person, interpersonal, network, and societal elements. guidelines emphasizing schooling exemplify the person degree, empowering ladies with knowledge approximately maternal fitness and properly-being. simultaneously, network-pushed initiatives like the approved Social Health Activist (ASHA) software perform on the interpersonal and community degrees. ASHAs, appearing as intermediaries, have interaction with neighbourhood communities, fostering awareness and facilitating get right of entry to healthcare offerings. by way of running at multiple stages, those interventions understand that person fitness is intricately connected to interpersonal relationships, community dynamics, and broader societal contexts (Khandale and Kedar, 2017). The Social Ecological version gives a complete framework, allowing interventions to goal numerous elements influencing maternal fitness and fostering a more holistic and interconnected approach to cope with this complicated public fitness trouble.
Health Belief Model
Purchaser-centered interventions, along with the Pradhan Mantri Surakshit Matritva Abhiyan (PMSMA), resonate with the concepts of the health belief version. consistent with this model, people are much more likely to interact in fitness-selling behaviours if they understand the severity of a health problem and accept as true with inside the blessings of particular actions. PMSMA, imparting free antenatal care, aligns with this angle through addressing perceived obstacles to searching for healthcare all through being pregnant. through putting off financial constraints and emphasizing personalized interest, the intervention enhances the perceived benefits of receiving antenatal care (inexperienced et al., 2020). This strategic alignment with the health faith model encourages pregnant ladies to prioritize and have interaction in critical healthcare practices, contributing to stepped forward maternal health outcomes through a client-centered method that considers character ideals and perceptions.
Critical Evaluation Using Various Lenses
Caplan and Holland’s Model
Caplan and Holland’s version underscores the significance of contextual appreciation in public fitness interventions. Exemplified by way of rules like the Janani Suraksha Yojana (JSY), this model emphasizes the need of considering cultural nuances and the socio-financial context while aiming to lessen maternal mortality. guidelines that fail to cope with these contextual elements risk unintentional outcomes, probably fostering elevated medicalization of childbirth. JSY, even as designed to beautify institutional deliveries, should navigate the complicated social panorama to make sure cultural sensitivity and inclusivity. via integrating cultural and socio-financial considerations, interventions can better align with the numerous needs of groups, promoting effectiveness at the same time as mitigating the threat of unintentional bad consequences (Caplan and Holland, 1990). This version encourages a nuanced technique, spotting that the fulfillment of interventions hinges on their compatibility with the social realities of the populations they purpose to serve.
Beattie’s Model
Beattie’s version offers insights into the dynamic spectrum among professional-led and participatory approaches in public fitness interventions. examining policies like the Janani Suraksha Yojana (JSY), which is predominantly professional-led, and network-driven initiatives just like the approved Social Health Activist (ASHA) application, Beattie’s model underscores the want for a delicate stability. JSY, pushed through top-down expertise, aims for considerable implementation but may additionally hazard be overlooking community-precise desires. In assessment, ASHA embraces a more participatory approach by way of attractive nearby communities in selling maternal fitness (Kanadia et al., 2006). To make certain the sustainability and effectiveness of interventions, finding equilibrium between expert guidance and network participation becomes essential. hanging this stability allows interventions to benefit from each the intensity of knowledge and the contextual richness provided by way of groups, fostering a synergistic and inclusive technique to address complicated public fitness demanding situations.
Consideration of Expert-Led vs. Participatory Approaches
Expert-Led Approaches:
Guidelines established by means of the Janani Suraksha Yojana (JSY), using a top-down approach, have the ability for good sized implementation. However, the chance lies in ability oversight of community-specific desires. For professional-led interventions like JSY to be powerful, flexibility and flexibility are essential. They need to well-known and deal with the specific demanding situations faced by means of various groups, making sure that the intervention remains contextually applicable and impactful.
Participatory strategies:
network-pushed tasks, typified by way of the accepted Social Health Activist (ASHA) program, empower local communities in selling maternal fitness. even as fostering empowerment, challenges in scalability and standardization may additionally stand up. hanging a stability between community participation and an established framework is essential. This ensures interventions, like ASHA, preserve cultural sensitivity whilst upholding effectiveness, creating a harmonious synergy between community engagement and organized implementation.
Ethical Considerations
It is important to consider the Nuffield Council on Bioethics’ “intervention ladder,” which is a framework for thinking about the acceptability and proportionality of different public health measures (PubMed, 2015). The ladder ranges from the least to the most intrusive interventions, with the idea that more intrusive interventions require stronger justification.
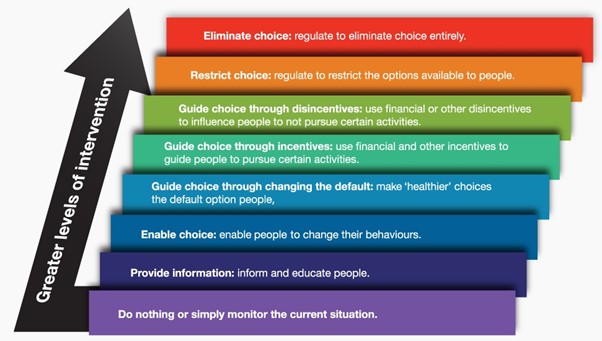
Source – BMC series blog
Ethical Considerations in Maternal Health Interventions
When applying the Nuffield ladder to maternal health in India, interventions can range from providing information and education about maternal health services to more coercive measures such as mandatory health checks. The ethical acceptability of these interventions depends on their ability to respect individual autonomy while achieving public health goals.
For instance, UNICEF’s efforts to increase access to quality maternal health services in India (UNICEF INDIA, 2019) can be seen as lower-rung interventions on the ladder, focusing on providing services and support without significantly infringing on individual autonomy. These interventions are generally considered ethically acceptable as they aim to improve health outcomes without restricting individual freedoms.
Victim Blaming and Respect for Autonomy
Victim blaming in the context of maternal health can occur when adverse outcomes are attributed to the individual’s failure to make the “right” choices, such as not hiring a doula or choosing the correct hospital (georgiabirth.org, 2015). This perspective fails to acknowledge the systemic issues that contribute to maternal mortality and morbidity, such as a lack of access to quality care, socioeconomic barriers, and institutional biases. Ethically, it is important to avoid victim blaming and instead focus on systemic interventions that can empower women and improve health outcomes without compromising respect for their autonomy.
Balancing Interests and Choice
The implementation of professional midwife-led maternity care in India is an example of an intervention that respects women’s autonomy by minimizing unnecessary interventions in pregnancy and labor. This aligns with the ethical principle of beneficence, which emphasizes the need to do good and avoid harm. It also respects the principle of autonomy by supporting informed choice and consent in maternity care.
The Role of Evidence in Ethical Public Health Practice
Policies should be based on the best available scientific evidence. However, evidence on the benefits and risks of public health policies is often incomplete or contested. Poor evidence should not be used as a reason for inaction, especially when inaction can have negative consequences for public health. This is particularly relevant in the context of maternity care in India, where there are high rates of interventions like cesarean sections in some states, and low rates of care in others, indicating a need for evidence-based practice.
Informed Consent:
In client-centered interventions, in particular in maternal health like the Pradhan Mantri Surakshit Matritva Abhiyan (PMSMA), securing informed consent is paramount. moral considerations demand that pregnant girls are not solely knowledgeable approximately their care preferences however actively engaged in choice-making approaches. This includes providing comprehensive statistics approximately antenatal care methods, ability dangers, and alternative options, allowing female to make independent picks aligned with their selections and values. Respecting the precept of knowledgeable consent no longer solely upholds ethical requirements but also contributes to building faith between healthcare vendors and pregnant female, fostering a collaborative and respectful technique to maternal care that values the autonomy and agency of the individuals concerned.
Ethical worries arise when interventions disproportionately advantage certain agencies. regulations have to be designed to cope with current inequities, ensuring that prone populations receive sufficient attention and sources.
Addressing maternal mortality in India necessitates a diverse range of interventions, every with its strengths and boundaries. relating those interventions to public health fashions, significantly evaluating them thru distinct lenses, and considering the balance between expert-led and participatory procedures are quintessential for growing comprehensive and sustainable techniques. ethical considerations guide the implementation of interventions, emphasizing the significance of equity, informed consent, and cultural sensitivity. ultimately, an included technique that recognizes the complexities of maternal health and engages groups in the process is fundamental for reaching significant and lasting discounts in maternal mortality prices.
Conclusion
IIn conclusion, addressing maternal mortality in India requires a complete and multifaceted approach grounded in public health theory, ethical concerns, and evidence-based interventions. A crucial aspect of this endeavor is the integration of healthcare assignments that strengthen maternal health services and ensure accessibility for all women. The vital analysis of interventions, ranging from client-focused to community-driven strategies, has illuminated both strengths and challenges. The alignment with public health models, including the Social Ecological model and the health belief model, ensures a holistic appreciation and targeted interventions. Ethical issues, guided by frameworks like the Nuffield ladder, emphasize the need for informed consent, equity, and cultural sensitivity. Striking a balance between professional-led and participatory methods is vital for sustainable interventions. The Caplan and Holland and Beattie’s models underscore the importance of contextual understanding and community engagement. To effectively reduce maternal mortality, healthcare assignments should be adaptive, inclusive, and responsive to the diverse needs of communities, reflecting a commitment to improving maternal health outcomes in India. Ultimately, enhancing healthcare delivery alongside community involvement will be key in fostering a supportive environment for maternal health.
Top Assignment Samples
Reference List
Alam, N., Mamun, M. and Dema, P., 2020. Reproductive, maternal, newborn, child, and adolescent health (RMNCAH): Key global public health agenda in SDG era. Good Health and Well-Being, pp.583-593.
Caplan, R. and Holland, R., 1990. Rethinking health education theory. Health Education Journal, 49(1), pp.10-12.
Das, S., 2018. Maternal health, human rights, and the politics of state accountability: Lessons from the Millennium Development Goals and implications for the Sustainable Development Goals. Journal of Human Rights, 17(5), pp.550-567.
Green, E.C., Murphy, E.M. and Gryboski, K., 2020. The health belief model. The Wiley encyclopedia of health psychology, pp.211-214.
Hamal, M., Dieleman, M., De Brouwere, V. and de Cock Buning, T., 2020. Social determinants of maternal health: a scoping review of factors influencing maternal mortality and maternal health service use in India. Public Health Reviews, 41(1), pp.1-24.
Jose, J., 2018. Reducing maternal mortality in India: A four-pronged strategy. Perspectives.
Kanadia, R.N., Shin, J., Yuan, Y., Beattie, S.G., Wheeler, T.M., Thornton, C.A. and Swanson, M.S., 2006. Reversal of RNA missplicing and myotonia after muscleblind overexpression in a mouse poly (CUG) model for myotonic dystrophy. Proceedings of the National Academy of Sciences, 103(31), pp.11748-11753.
Khandale, S.N. and Kedar, K., 2017. Analysis of maternal mortality: a retrospective study at tertiary care centre. International Journal of Reproduction, Contraception, Obstetrics and Gynecology, 6(4), pp.1610-1614.
Kumari, K., Srivastava, R.K., Srivastava, M. and Purwar, N., 2019. Maternal mortality in rural Varanasi: delays, causes, and contributing factors. Indian journal of community medicine: official publication of Indian Association of Preventive & Social Medicine, 44(1), p.26.
Meh, C., Sharma, A., Ram, U., Fadel, S., Correa, N., Snelgrove, J.W., Shah, P., Begum, R., Shah, M., Hana, T. and Fu, S.H., 2022. Trends in maternal mortality in India over two decades in nationally representative surveys. BJOG: An International Journal of Obstetrics & Gynaecology, 129(4), pp.550-561.
Mukaruzima, L., Duhamahoro, J. and Frantz, J.M., 2023. Stakeholder perspectives on promoting health enhancing sport through the Rwanda Sports Policy. International Journal of Sport Policy and Politics, 15(4), pp.619-633.
O’Neil, S., Vohra, D. and Pottinger, E., 2019. Building Coalitions to Support Maternal Health Quality of Care in India (No. 1dde00926911405cad3ec1376de0646d). Mathematica Policy Research.
Parsekar, S.S., Pundir, P. and Bevilacqua, V., 2020. Reproductive, maternal, Newborn, child and adolescent health and related behaviour change communication strategies in Bangladesh, Nepal and India: a narrative review. Clinical Epidemiology and Global Health, 8(1), pp.280-286.
Patrick, M., Afzal, G., Mahsud, M. and Hanifatu, M.N., 2022. Factors that affect maternal mortality in Rwanda: A comparative study with India and Bangladesh. Computational and Mathematical Methods in Medicine, 2022.
Prinja, S., Gupta, A., Bahuguna, P. and Nimesh, R., 2018. Cost analysis of implementing mHealth intervention for maternal, newborn & child health care through community health workers: assessment of ReMIND program in Uttar Pradesh, India. BMC Pregnancy and Childbirth, 18, pp.1-16.
Rajwar, E., Pundir, P., Parsekar, S.S., DS, A., D’Souza, S.R., Nayak, B.S., Noronha, J.A., D’Souza, P. and Oliver, S., 2023. The utilization of systematic review evidence in formulating India’s National Health Programme guidelines between 2007 and 2021. Health Policy and Planning, 38(4), pp.435-453.
Singh, G.K., 2021. Trends and social inequalities in maternal mortality in the United States, 1969-2018. International Journal of Maternal and Child Health and AIDS, 10(1), p.29.
Singla, A., Rajaram, S., Mehta, S. and Radhakrishnan, G., 2017. A ten year audit of maternal mortality: Millennium development still a distant goal. Indian journal of community medicine: official publication of Indian Association of Preventive & Social Medicine, 42(2), p.102.
Small, M.J., Allen, T.K. and Brown, H.L., 2017, August. Global disparities in maternal morbidity and mortality. In Seminars in perinatology (Vol. 41, No. 5, pp. 318-322). WB Saunders.
World Health Organization, 2018. Implementation guidance: protecting, promoting and supporting breastfeeding in facilities providing maternity and newborn services: the revised baby-friendly hospital initiative.