Introduction
Diabetic foot ulcers (DFUs) are a dire challenge, especially among the senior citizens. Researchers have found that distal ulcers have a more difficult time healing compared to proximal ones. Investigations into elderly patients with DFUs in outpatients, however, usually do not reveal the exact anatomic locations (Paisey et al., 2019). One of the main factors related to the DFU gravity is the increasing age. Old patients in the outpatient ambulatory care centres are especially prone to arise from the complications of DFUs because of the reduced mobility, impaired circulation and sensory neuropathy (Armstrong et al., 2023). Issues of DFUs are not only prevalent but also exhibit an imminent threat to healthcare systems with the elderly being at a higher risk of mortality and morbidity associated with non-healing ulcers (Boulton, 2019).
Compliance of various ages reveals distinct differences in outbreaks of DFU. Through a retrospective cohort study carried out in a Diabetic Foot Unit, a differentiation between younger and old DFU patients (18-64 years and ≥65 years, respectively) was demonstrated as the group with older adults had a 71.4 % incidence while the other group had an incidence of 43.4% among a sample of 435 patients (Rosinha et al., 2022).
Strikingly, the neuro-ischemic type of the DFUs were predisposed to the elderly population, revealing the importance of age-associated factors in the development and presentation of the ulcers as the older adults group had 71.4 % more frequent incidence of neuro-ischemic DFU compared to younger patients.
The available literature emphasizes the relevance of age in determining the outcomes of DFU. Studies presented differences in age-related DFU locations and severity, stressing the importance of developing target specific interventions designed for elderly people (Sorber and Abularrag, 2021). Nevertheless, elucidating the specific pathways of aging in relation to DFU subtype presentations requires additional research to allow for targeted treatment approaches.
Within the context of the public health field, the project is in line with the prevention measures intended to better the quality of care and health for those who are at the risk of developing challenges. This project offers a targeted solution to the issues of the current DFU management plans as specific aging people are considered and the national health agenda aims at reducing the burden of chronic wounds and improving patient outcomes in the elderly.
Project Initiation
Force Field Analysis
Force Field Analysis is a strategic element that is utilized in project initiation to evaluate the potential viability and implement ability of proposed interventions (Swanson and Creed, 2014). Through this analysis, the driving forces of this diabetic foot ulcers (DFUs) education for elderly patients in care homes are identified, as well as the factors that could restrain it. This tension between the competing forces determines the possibility that a project will be successful.
The net score from driving and restraining forces indicates whether the project is generally sustainable and viable. This report becomes the basis for the decision-making that sets a foundation for the needed focus and approaches for the removal of the implementation hurdles. The net score of the driving forces of 31 indicates that the project can be executed with a higher likelihood of success.
| Driving Forces | Score | Restraining Forces | Score |
| Increased awareness of the importance of DFU education | 7 | Limited resources for educational materials | 5 |
| Support from healthcare providers | 8 | Resistance to change among staff | 6 |
| Positive outcomes associated with patient education | 9 | Lack of prioritization of DFU education within units | 4 |
| Government policies promoting patient education | 7 | Time constraints for staff to deliver education | 5 |
| Total Driving Forces: 31 | Total Restraining Forces: 20 |
Table 1: Force Field Analysis
(Source: Self-developed)
Top UK Assignment Cities
Lewin’s Change Model
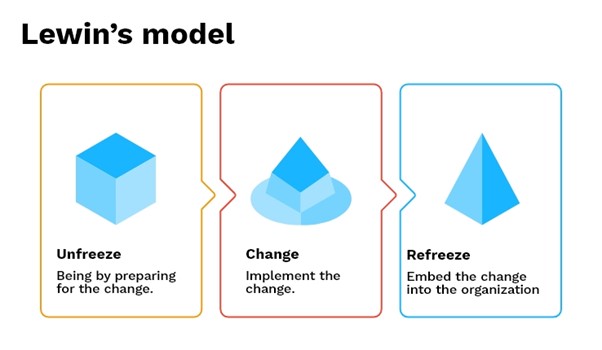
Figure 1: Lewin’s Change Management Model
(Source: Hussain et al., 2018)
Lewin’s three-stage change model, which consists of unfreezing, changing, and refreezing, provides the structured way of implementations of the revolution plans such as by improving the quality of patient education on DFU in the elderly care units (Hussain et al., 2018).
- Unfreezing: In the first place, the process of changing the existing situation includes the creation of awareness of the need for changes in the community as well as dealing with the potential barriers to change in terms of a lack of resources and resistance to change among staff (Burnes, 2020). It will involve the stakeholder at the early stage and educate the players on the importance of DFU education and call for the cooperation of the health care professionals.
- Changing: While in this phase, driving forces including population awareness and favourable outcomes from patient education are leveraged to adopt interventions and educational campaigns adequately. Stakeholders do not stand aloof from the change process, in fact, they are involved in overcoming challenges like time constraint and prioritization.
- Refreezing: The last stage involves establishing a solid base for the achieved changes by framing stable government policies and healthcare institutions’ priorities around DFU knowledge and education in the field of elderly care (Burnes, 2020). This stage targets to maintain the good outcomes performed and make them a permanent part of the routine healthcare practice.
Top UK Assignment Samples
Fishbone Analysis

Figure 2: Fishbone Diagram
(Source: Self-developed on Canva)
The Fishbone Analysis, or Ishikawa or cause-and-effect diagram, is a structured approach by which we identify the root causes of complex problems (Liliana, 2016). The use of the Fishbone Analysis in the context of the patient education on diabetic foot ulcers (DFUs) in elderly care units allows for the uncovering of factors deepening from the main problem hindering the implementation of the project. Fishbone Analysis involves total examination of factors affecting patient education programs successfully (Carvalho et al., 2021). Through an identification of five major groups of restraining forces: process/methods, people/staff, policies, equipment/resources, environment and external factors healthcare professionals can define the exact areas that need to be adjusted. This systematic approach strengthens the facility to solve problems and help in the determination of precise strategies to attack the root causes.
Get Assignment Help for Top Subjects
Goal and Objectives
The objectives of the project developed are designed to solve the problems pointed out and get advantage of the opportunities found through the force field and fishbone analyses with consideration of SMART criteria for progress.
- Objective 1: Creating patient education protocols that are standardized.
- SMART Goal: By the end of three months, create and implement standardized instructional guidelines for the elderly patients of DFUs in care units. The key is maintaining a high level of consistency and quality in delivery of education.
- Objective 2: Upgrade Staff Training Courses on DFU Education.
- SMART Goal: Within 5 months, organize comprehensive classes for the healthcare personnel about effective patient teaching regarding DFUs covering the topics of wound care, risk factors, and prevention.
- Objective 3: Set up Collaborative Frameworks for Education in DFU.
- SMART Goal: Within the 6 months, in collaboration with unit management, integrate the DFU education into the current formats by ensuring the sustainability and the priority of the educational initiatives in the process.
- Objective 4: Provide easy access to educational resources
- SMART Goal: During this period, purchase and deliver instructional resources such as print material and digital tools, in order to guarantee accessibility and teaching patients about the diabetic foot ulcer in the old people’s care facilities.
Feeling Overwhelmed By Your Assignment?
Get assistance from our PROFESSIONAL ASSIGNMENT WRITERS to receive 100% assured AI-free and high-quality documents on time, ensuring an A+ grade in all subjects.
Stakeholder Identification
Such project which is concerned with promoting patient education on diabetic foot ulcers (DFUs) in elderly care units, diverse stakeholders do play significant roles in this process. These stakeholders are a mix of individuals and organizations and each one has different interpretations, perspectives and conflicts (McDermott et al., 2023).
Healthcare Providers: Healthcare providers working at the front line such as nurses, doctors and podiatrists are commonly in charge of teaching patient on the care of DFUs (Coffey et al., 2019). Their purpose is all about offering holistic care to patients and enhancing patients’ health. On the contrary, challenges in implementation might be discovered as a result of the time factor, competing priorities, and education practice inertia.
Management/Administration: Unit managers, directors and administrators on the other side seek to achieve effective utilisation of resources, compliance with regulations and reputation of the organisation (Grennan, 2019). Confrontations will emerge due to budget constraints, conflict of priorities, and resisting change of policies regarding the workflow.
Patients and Families: Patients and their families strive to gain information, power, and better health outcomes when they are educated on DFUs and its management (Wang et al., 2022). Nevertheless, divergent levels of health literacy, cultural practices, and availability of health care structures are the possible barriers to be anticipated.
External Stakeholders: External stakeholders like governmental bodies, healthcare regulators, and community organisations may have interests in effective management of public health campaigns, assurance of standards, allocation of fund etc (Jalilian et al., 2020).
| Stakeholder | Interests | Potential Conflicts | Beneficiaries | Investors |
| Healthcare Providers | Delivering comprehensive care | Time constraints, resistance to change | Patients, healthcare system | Healthcare system |
| Management/Admin | Efficient resource allocation, regulatory compliance | Budget constraints, conflicting priorities | Patients, healthcare system | Healthcare system, investors |
| Patients and Families | Knowledge, empowerment, improved health outcomes | Varying health literacy, cultural beliefs | Patients, families | Healthcare system |
| External Stakeholders | Promoting public health initiatives, ensuring quality standards | Resource allocation, regulatory compliance, competing agendas | Patients, community | Healthcare system, community |
Table 2: Stakeholder Management Plan
(Source: Self-developed)
Project Planning & Feasibility
Major Activities
Developing the project of delivering education concerning diabetic foot ulcers (DFUs) to the patients in nursing homes need a well-defined plan in which activities are specifically stated, and the roles and tasks are clearly assigned.
Main Activities and Interventions
- Development of Standardised Educational Protocols: Formulating a research-based patient instruction pertaining to DFUs, which consists of an understanding of wound care, associated risk factors, and preventive measures (Jalilian et al., 2020).
- Staff Training and Capacity Building: Hold learning sessions for the health workers to get the fundamental concepts and techniques about instructing injured patients (Van Netten et al., 2020).
- Procurement and Distribution of Educational Resources: Provision of teaching materials such as print materials and digital tools which is later transported to health centers to let patients know more about their conditions (Edmonds et al., 2021).
- 4. Policy Development and Integration: Through coordination with organizational managers, DFU education gradually becomes part of the existing tools and procedures, ensuring that DFU education is part of normal business operations (Monteiro‐Soares et al., 2020).
- Stakeholder Engagement and Communication: Establishing transparent communication channels and engaging all stakeholders at all levels to garner as much support as possible, address concerns, and foster cooperation and collaboration throughout the project implementation process (van Netten et al., 2019).
Resource and Responsibility Allocation
- Human Resources: Well-trained educators, doctors, managers responsible for developing educational content, running coaching classes and coordination of project activities (Monteiro‐Soares et al., 2020).
- Material Resources: Teaching materials, digital resources delivering facilities, and the training arrangements and the meetings places for the stakeholders (Messenger et al., 2019).



Development of Gantt Chart
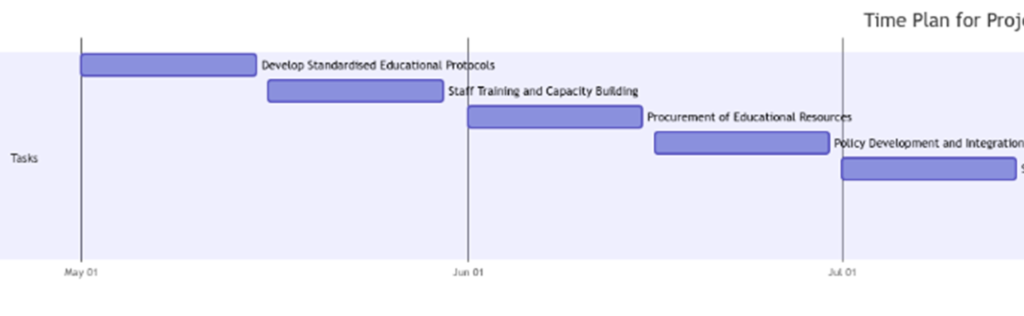
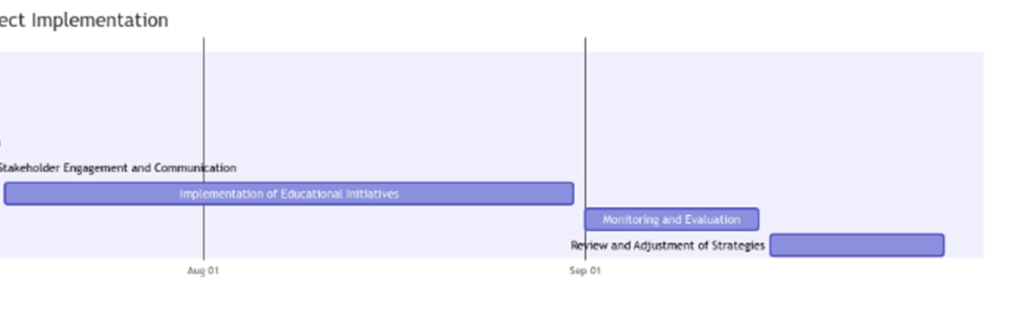
Figure 3: Gantt Chart
(Source: Refer to Appendix A)
The devised schedule explains a systematic way of the activities staged for elderly care units with a goal of improving patients’ knowledge on DFUs (Ramachandran and Karthick, 2019). The project would be launched in May 2024, with the initial phase focusing on drafting standard protocols for education, thereby guaranteeing uniformity and high quality across all educational methods.
As next, healthcare workers attend training and capacity building sessions between mid-May and the end of the month to build the indispensable knowledge and skills that they will need for efficient patient education. Then the organization is responsible for getting educational resources, developing polices and integrating policies and stakeholder engagement and communication that finally lead to the implementation phase.
The longer phase of implementing educational initiatives starts in mid-July and runs until the end of August, providing enough time for the implementation of educational programs and interventions in elderly care homes. The monitoring and evaluation activities should be carried out in September to ensure the assessment of project outcomes and the identification of areas for need of improvement. Thus, the time plan has a review and adjustment of strategies towards the end of September towards perfecting the approach of patient education (Shibuya, M. and Chen, 2021).
Risk Analysis and Mitigation Strategies
The important point in this project which is focused on improving diabetes patient education on diabetic foot ulcers (DFU) in elderly care homes is to spot out the risks and derive effective mitigation strategies.
- Resource Constraints: Raising money for purchasing instructional materials could be another challenge along with workshops for staff members (Kim and Han, 2020).
- Resistance to Change: The hesitancy of nurse practitioners and other medical staff in adapting these DFU educational protocol or including such information in their professional practices (Abrar et al., 2020) is worth mentioning.
- Time Constraints: Tight deadlines however can give rise to tasks which are unfinished in turn reducing the quality of deliverables or sometimes even leading to project noncompletion (Hicks et al., 2020). Mittigation tactics would include time management, task prioritization based on the urgency and the impact, and also have contingency planning as a backup in case of delays.
- Lack of Stakeholder Buy-in: One of such barriers is low level of the active participation and support from main stakeholders, which include providers, managers and patients (Nguyen et al., 2019).
- External Factors: Uncertainty could be the result of various factors that are outside the project as policies get amended, changes in health care policies take place or, for example, pandemics overwhelm the project (Dayya et al., 2022).
| Risk | Likelihood | Impact | Mitigation Strategies |
| Resource Constraints | High | High | Seek alternative funding sources. Establish partnerships with external organisations for resource sharing. Prioritise resource allocation based on critical project needs. |
| Resistance to Change | Medium | High | Engage stakeholders through clear communication and education on the benefits of proposed changes. Provide continuous support and training to facilitate transition. |
| Time Constraints | High | Medium | Implement careful time management practices. Prioritise tasks based on urgency and impact. Develop contingency plans to address unforeseen delays. |
| Lack of Stakeholder Buy-in | Medium | High | Foster open communication channels with stakeholders. Address concerns and feedback promptly. Demonstrate project value through tangible outcomes and benefits. |
| External Factors (e.g., regulatory changes, pandemics) | Low | High | Maintain flexibility and adaptability in project planning. Establish contingency plans to address unforeseen events. Stay informed of external developments and adjust plans accordingly. |
Table 3: Risk Management Plan
(Source: Self-developed)
Stakeholder Prioritisation and Communication Plan
Stakeholder focus influences better communication and hence incorporation of handling DFU problem in the elderly care units. Healthcare providers, management and administration division, patients and their relatives, and external parties like government bodies and local communities are the most important stakeholders as they are either directly involved in or control project outcomes.
Communication Strategies among Various Stakeholders
- Healthcare Providers: Have a team meeting, send e-mail updates, and create a training session into the dissemination of the project progress, collect feedback and solve the problem associated with education system transformation and initiatives (Lo et al., 2021).
- Management/Administration: Conduct formal presentations, written reports, and one on one meetings to illustrate project milestone progress, resources allocation, as well as policy integration successes (Dixon & Edmonds, 2021)..
- Patients and Families: Emphasize patient education using patient education materials, informational sessions, and interactive workshops as tools to empower patients and their families with knowledge on DFUs, treatment options, and self-care practices (Huang et al., 2019).
- External Stakeholders: Attend collaborative meetings, policy forums, and networking events in order to tailor objectives of a project with the whole public health system, ask for support during resource mobilization and meet regulatory requirements (Goodall et al., 2020).
Communication and Engagement Plan
| Stakeholder | Communication Content | Frequency | Communication Method |
| Healthcare Providers | Project progress updates, feedback solicitation | Weekly | Team meetings, email updates |
| Management/Admin | Project milestones, resource allocation, policy updates | Monthly | Formal presentations, written reports |
| Patients and Families | DFU education, treatment options, self-care practices | As needed | Patient education materials, workshops |
| External Stakeholders | Project alignment with public health initiatives | Quarterly | Collaborative meetings, policy forums |
Table 4: Stakeholder Communication and Engagement Plan
(Source: Self-developed)
Project Implementation and Monitoring
Transition to Implementation
The transition from planning to action is the milestone for our project led to improving patient education of diabetic foot ulcers in elderly care facilities. Now, the actual work begins as the details are ironed out and the resources are allocated; strategies laid in the project plan have to align with the objectives and stakeholder’s expectations.
Implementation and Monitoring Process
Leadership that propels project teams through the implementation process is absolutely crucial. This participative leadership approach involving cooperative decision making and team member empowerment which builds up engagement and ownership is encouraged (Goodall et al., 2020). This practice helps to empower medical professionals to play their share in teaching patients about DFUs and, in the process, create a feeling of responsibility and investment in the project.
Gantt Chart and Communication in Real Situation
Using a Gantt chart not only provides the visualisation of the project milestones, tasks and the dependencies between them but the monitor of the progress and potential bottlenecks as well (Nally and Waters, 2022). Continuous communication, calendar and informal, ensures the coordination of team efforts and the transparency of reporting progress. Recurrent team meetings, progress reports, and e-mails are community practices for information sharing, problem solving, and suggestions from team members.
Dealing with Time Delays or Resource Problems
In a case where there are stalls or shortcomings in resources, the project managers need to evaluate the impact on the project timeframe as well as communication channels. Timely communication in the form of delays notification or resource constraints enable stakeholders to be aligned with their expectations and distribute their resources rightly (Akindote et al., 2024). Agility in project planning is a vital precondition to redistribution of resources and readjustment of deadlines. Such moves are intended to avoid damage to project deliverables.
Risk Scenario Response
Strategizing the responses to potential risks demands proactive leadership and effective communication. A situation of resource constraints compels project managers to involve stakeholders in the search for alternative sources of funding and reallocating the resources to the mission critical project areas (Abyad, 2021). The process of explaining the reasons for the changes and the anticipated consequences on project outcome enhance comprehension and cooperation among the stakeholders. Where there is a strong resistance to change, leaders need to use clear and persuasive communication strategies so that they can point out the benefits of the proposed changes and respond to the questions and concerns raised by stakeholders (Dash et al., 2019).
Project Evaluation
Evaluation Purpose
The goal of project evaluation is to find out how successful the objectives of patient education regarding diabetic foot ulcers (DFUs) are in the old people’s home. Evaluation provides insights on the effectiveness of the plan, pinpoints areas of improvement and makes informed future decision-making (Sipes, 2023). The principal purpose of evaluation is to find out the impact of educational initiatives on patient knowledge including their self-care practices, evaluate the efficiency of communication and leadership approaches employed during project implementation and discover the lessons learnt for use in similar initiatives.
Data and Information Requirements
The type of data and information that is needed to measure whether the project objectives are being met is patient outcomes data, pre- and post-intervention surveys which assess patient knowledge and behavior related to DFUs, document of feedback from healthcare providers and stakeholders, as well as the evidence of project activities and milestones (Giasson, 2019). Examples of data sources include patient records, survey responses, meeting minutes, progress reports, and communication logs. Another important aspect is qualitative data which is composed of patient testimonials, and stakeholder interviews as this way may help to get a general picture of the effectiveness of educational interventions, and communication strategies.
Effectiveness Assessment
The effectiveness of communication and leadership styles utilized during the implementation of the project will be examined using a mix of qualitative and quantitative approaches. Quantitative data from team members, stakeholders, and patients will be solicited to assess aspects of communication effectiveness, the adaptability of leadership approaches, and the overall project management (Collier and Breeden, 2023). Quantitative assessment including monitoring of project deadlines achievement, milestones attainment, and behavioural changes in patient knowledge will be undertaken to reveal the impact of communication and leadership styles on the project outcomes.
Project Limitations
Even though the project will be meticulously planned and carried out, the initial constraints and the project limitations may however influence the final outcomes. Firstly, limitations to the generalisability of findings are likely to occur due to the singularity of elderly care units and the specified population with their own unique qualities (White et al., 2019). For the second part, external factors like policy changes and shortage of funding in healthcare may alter the projects and the expected outcome. Furthermore, the issue of self-reported data and subjective measures of performance and the impact they have on the reliability of the evaluation results is also valid. Also, the fact that this is short-term project will not allow to assess long-term sustainability and permanence of intervention outcomes (Nally and Waters, 2022). It is pertinent to be aware of these limitations and assess the evaluation findings against this context to gain a full understanding of the project impacts as well as to establish a basis for future enhanced projects.
Conclusion
The impact of this project on elderly care units which concentrated on the knowledge of DFUs among patients carries great importance for forming one’s personality and further professional environment. The participants have obtained proficiency in project management, mutual engagement with the stakeholders and the communication within the healthcare environment due to being involved in different phases of the project. These interactions have proven to be the invaluable lessons, which enable the participants to face and deal with different complicated challenges and make a significant difference in their positions.
Besides, there are perspective points gained that can be applied elsewhere within the healthcare system. As the established success factors entail the role of stakeholder engagement, individualized communication strategies, and efficient leadership methods, they can all be transferred to programs aiming to address various patients’ groups and illnesses. Emphasizing on pursuing evidence-based practices and regular evaluation as a framework for creating and implementing strong educational programmes in numerous healthcare facilities can be a benchmark.
References
Abrar, E.A., Yusuf, S., Sjattar, E.L. and Rachmawaty, R. (2020). Development and evaluation educational videos of diabetic foot care in traditional languages to enhance knowledge of patients diagnosed with diabetes and risk for diabetic foot ulcers. Primary care diabetes, 14(2), pp.104-110. https://doi.org/10.1016/j.pcd.2019.06.005
Abyad, R. (2021). The role of project management in public health. World Fam. Med, 19, pp.87-96. http://www.mejfm.com/May%202021/WFM%20May2021.pdf#page=87
Akindote, O.J., Adegbite, A.O., Omotosho, A., Anyanwu, A. and Maduka, C.P. (2024). Evaluating the effectiveness of it project management in healthcare digitalization: a review. International Medical Science Research Journal, 4(1), pp.37-50. https://doi.org/10.51594/imsrj.v4i1.698
Armstrong, D.G., Tan, T.W., Boulton, A.J. and Bus, S.A. (2023). Diabetic foot ulcers: a review. Jama, 330(1), pp.62-75. https://doi.org/10.1001/jama.2023.10578
Boulton, A.J. (2019). The diabetic foot. Medicine, 47(2), pp.100-105. https://doi.org/10.1016/j.mpmed.2018.11.001
Burnes, B. (2020). The origins of Lewin’s three-step model of change. The Journal of Applied Behavioral Science, 56(1), pp.32-59. https://doi.org/10.1177/0021886319892685
Carvalho, R., Lobo, M., Oliveira, M., Oliveira, A.R., Lopes, F., Souza, J., Ramalho, A., Viana, J., Alonso, V., Caballero, I. and Santos, J.V. (2021). Analysis of root causes of problems affecting the quality of hospital administrative data: A systematic review and Ishikawa diagram. International journal of medical informatics, 156, p.104584. https://www.sciencedirect.com/science/article/pii/S1386505621002100
Coffey, L., Mahon, C. and Gallagher, P. (2019). Perceptions and experiences of diabetic foot ulceration and foot care in people with diabetes: a qualitative meta‐synthesis. International wound journal, 16(1), pp.183-210. https://doi.org/10.1111/iwj.13010
Collier, S. and Breeden, E. (2023). Introducing project management to student pharmacists in a healthcare informatics course. Pharmacy Education, 23(1), pp.755-761. https://doi.org/10.46542/pe.2023.231.755761
Cummings, S., Bridgman, T. and Brown, K.G., 2016. Unfreezing change as three steps: Rethinking Kurt Lewin’s legacy for change management. Human relations, 69(1), pp.33-60. https://doi.org/10.1177/0018726715577707
Dash, S., Shakyawar, S.K., Sharma, M. and Kaushik, S. (2019). Big data in healthcare: management, analysis and future prospects. Journal of big data, 6(1), pp.1-25. https://doi.org/10.1186/s40537-019-0217-0
Dayya, D., O’Neill, O.J., Huedo-Medina, T.B., Habib, N., Moore, J. and Iyer, K. (2022). Debridement of diabetic foot ulcers. Advances in wound care, 11(12), pp.666-686. https://doi.org/10.1089/wound.2021.0016
Dixon, D. and Edmonds, M. (2021). Managing diabetic foot ulcers: pharmacotherapy for wound healing. Drugs, 81(1), pp.29-56. https://doi.org/10.1007/s40265-020-01415-8
Edmonds, M., Manu, C. and Vas, P. (2021). The current burden of diabetic foot disease. Journal of clinical orthopaedics and trauma, 17, pp.88-93. https://doi.org/10.1016/j.jcot.2021.01.017
Giasson, L. (2019). The Best of Both Models: Key Components of a Successful Hybrid Project Management Office Model in a Health Care Organization. The health care manager, 38(3), pp.247-252. https://doi.org/10.1097/HCM.0000000000000272
Goodall, R.J., Ellauzi, J., Tan, M.K., Onida, S., Davies, A.H. and Shalhoub, J. (2020). A systematic review of the impact of foot care education on self efficacy and self care in patients with diabetes. European Journal of Vascular and Endovascular Surgery, 60(2), pp.282-292. https://doi.org/10.1016/j.ejvs.2020.03.053
Grennan, D. (2019). Diabetic foot ulcers. Jama, 321(1), pp.114-114. https://doi.org/10.1001/jama.2018.18323
Hicks, C.W., Canner, J.K., Mathioudakis, N., Lippincott, C., Sherman, R.L. and Abularrage, C.J. (2020). Incidence and risk factors associated with ulcer recurrence among patients with diabetic foot ulcers treated in a multidisciplinary setting. Journal of Surgical Research, 246, pp.243-250. https://doi.org/10.1016/j.jss.2019.09.025
Huang, Z.H., Li, S.Q., Kou, Y., Huang, L., Yu, T. and Hu, A. (2019). Risk factors for the recurrence of diabetic foot ulcers among diabetic patients: a meta‐analysis. International wound journal, 16(6), pp.1373-1382. https://doi.org/10.1111/iwj.13200
Hussain, S.T., Lei, S., Akram, T., Haider, M.J., Hussain, S.H. and Ali, M. (2018). Kurt Lewin’s change model: A critical review of the role of leadership and employee involvement in organizational change. Journal of innovation & knowledge, 3(3), pp.123-127. https://doi.org/10.1016/j.jik.2016.07.002
Jalilian, M., Ahmadi Sarbarzeh, P. and Oubari, S. (2020). Factors related to severity of diabetic foot ulcer: a systematic review. Diabetes, Metabolic Syndrome and Obesity, pp.1835-1842. https://doi.org/10.2147/DMSO.S256243
Kim, E.J. and Han, K.S. (2020). Factors related to self‐care behaviours among patients with diabetic foot ulcers. Journal of Clinical Nursing, 29(9-10), pp.1712-1722. https://doi.org/10.1111/jocn.15215
Liliana, L., 2016, November. A new model of Ishikawa diagram for quality assessment. In Iop conference series: Materials science and engineering (Vol. 161, No. 1, p. 012099). IOP Publishing. https://doi.org/10.1088/1757-899X/161/1/012099
Lo, Z.J., Surendra, N.K., Saxena, A. and Car, J. (2021). Clinical and economic burden of diabetic foot ulcers: a 5‐year longitudinal multi‐ethnic cohort study from the tropics. International wound journal, 18(3), pp.375-386. https://doi.org/10.1111/iwj.13540
McDermott, K., Fang, M., Boulton, A.J., Selvin, E. and Hicks, C.W. (2023). Etiology, epidemiology, and disparities in the burden of diabetic foot ulcers. Diabetes Care, 46(1), pp.209-221. https://doi.org/10.2337/dci22-0043
Messenger, G., Taha, N., Sabau, S., AlHubail, A. and Aldibbiat, A.M. (2019). Is there a role for informal caregivers in the management of diabetic foot ulcers? A narrative review. Diabetes Therapy, 10, pp.2025-2033. https://doi.org/10.1007/s13300-019-00694-z
Monteiro‐Soares, M., Boyko, E.J., Jeffcoate, W., Mills, J.L., Russell, D., Morbach, S. and Game, F. (2020). Diabetic foot ulcer classifications: a critical review. Diabetes/metabolism research and reviews, 36, p.e3272. https://doi.org/10.1002/dmrr.3272
Monteiro‐Soares, M., Russell, D., Boyko, E.J., Jeffcoate, W., Mills, J.L., Morbach, S., Game, F. and International Working Group on the Diabetic Foot (IWGDF) (2020). Guidelines on the classification of diabetic foot ulcers (IWGDF 2019). Diabetes/metabolism research and reviews, 36, p.e3273. https://doi.org/10.1002/dmrr.3273
Nally, R. and Waters, G. (2022). Project Management: Enabling Communication and Healthcare IT Implementations. In Nursing Informatics: A Health Informatics, Interprofessional and Global Perspective (pp. 559-568). Cham: Springer International Publishing. https://doi.org/10.1007/978-3-030-91237-6_36
Nguyen, T.P.L., Edwards, H., Do, T.N.D. and Finlayson, K. (2019). Effectiveness of a theory-based foot care education program (3STEPFUN) in improving foot self-care behaviours and foot risk factors for ulceration in people with type 2 diabetes. Diabetes research and clinical practice, 152, pp.29-38. https://doi.org/10.1016/j.diabres.2019.05.003
Paisey, R.B., Abbott, A., Paisey, C.F., Walker, D., Birch, R., Bowen, B., Brown, R., Clark, C., Collings, R., Cutts, S. and Davies, J. (2019). Diabetic foot ulcer incidence and survival with improved diabetic foot services: an 18‐year study. Diabetic Medicine, 36(11), pp.1424-1430. https://doi.org/10.1111/dme.14045
Rosinha, P., Saraiva, M., Ferreira, L., Garrido, S., Carvalho, A., Freitas, C., Amaral, C., Costa, L., Loureiro, L., Carvalho, R. and de Carvalho, A.C. (2022). A retrospective cohort study on diabetic foot disease: ascertainment of ulcer locations by age group. Cureus, 14(8). https://doi.org/10.7759/cureus.28189
Sipes, C. (2023). Project management for the advanced practice nurse. Springer Publishing Company. https://books.google.com/books?hl=en&lr=&id=I5HYEAAAQBAJ&oi=fnd&pg=PP1&dq=Sipes,+C.+(2023).+Project+management+for+the+advanced+practice+nurse.+Springer+Publishing+Company.&ots=x4NS3iEsAz&sig=n9htIi7qmh0bFT-k-EeYlQUIBbo
Sorber, R. and Abularrage, C.J. (2021), March. Diabetic foot ulcers: epidemiology and the role of multidisciplinary care teams. In Seminars in vascular surgery (Vol. 34, No. 1, pp. 47-53). WB Saunders. https://doi.org/10.1053/j.semvascsurg.2021.02.006
Swanson, D.J. and Creed, A.S., 2014. Sharpening the focus of force field analysis. Journal of change management, 14(1), pp.28-47. https://doi.org/10.1080/14697017.2013.788052
van Netten, J.J., Seng, L., Lazzarini, P.A., Warnock, J. and Ploderer, B. (2019). Reasons for (non‐) adherence to self‐care in people with a diabetic foot ulcer. Wound Repair and Regeneration, 27(5), pp.530-539. https://doi.org/10.1111/wrr.12728
Wang, X., Yuan, C.X., Xu, B. and Yu, Z. (2022). Diabetic foot ulcers: Classification, risk factors and management. World journal of diabetes, 13(12), p.1049. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9791567/
White, K.M., Dudley-Brown, S. and Terhaar, M.F. eds. (2019). Translation of evidence into nursing and healthcare. Springer Publishing Company.https://books.google.com/books?hl=en&lr=&id=1faVDwAAQBAJ&oi=fnd&pg=PP1&dq=White,+K.M.,+Dudley-Brown,+S.+and+Terhaar,+M.F.+eds.+(2019).+Translation+of+evidence+into+nursing+and+healthcare.+Springer+Publishing+Company.&ots=FFvkmS6W2O&sig=tchqDqSaER7ZygenKLyC7xfhPH4
Explore Recent Blogs
-
How to Write a Detailed Report: From Planning to Polishingby arora.vijay27jan on January 29, 2026
A detailed report represents critical research and professional competency. Reports provide readers with a comprehensive understanding of the information presented in a coherent format. In addition to reporting the details of a specific situation or… The post How to Write a Detailed Report: From Planning to Polishing first appeared on Digi Assignment Help.
-
How to Write an Assignment on the First Pageby arora.vijay27jan on January 13, 2026
Mastering the skill of writing assignments is one of the most essential academic skills for every student. While most focus on what is contained in the body of the assignment, students frequently overlook the significance… The post How to Write an Assignment on the First Page first appeared on Digi Assignment Help.
-
Most Controversial Debate Topics To Win Any Argumentby arora.vijay27jan on January 12, 2026
Debates are not simply casual conversations about what you think or feel on a specific subject, but rather well-organised and structured forms of discourse in which opposing sides analyse and defend their respective opinions, using… The post Most Controversial Debate Topics To Win Any Argument first appeared on Digi Assignment Help.
-
Significance Of Report Writingby arora.vijay27jan on January 9, 2026
The report is an important part of academic and professional life because it allows individuals to document information systematically, clearly, and indiscriminately so readers can make informed decisions about how to utilise that information for… The post Significance Of Report Writing first appeared on Digi Assignment Help.
-
How to Write a Hypothesis? Step-by-Step Guide with Examplesby Amelia on January 2, 2026
Many students must have experienced the “appear or disappear” situation when formulating a hypothesis for a new research venture. You are certainly not alone if you embark on a new research project and are unsure… The post How to Write a Hypothesis? Step-by-Step Guide with Examples first appeared on Digi Assignment Help.
-
How to Choose the Right Nursing Topic for Your Final-Year Projectby Amelia on July 8, 2025
Nursing is a competitive course offering a promising career for students. It is rigorous and demands up to date knowledge of the subject, good assignment writing, and field practice. Hence scoring good marks in nursing… The post How to Choose the Right Nursing Topic for Your Final-Year Project first appeared on Digi Assignment Help.